



Experts reveal hidden sign of kidney cancer
Fri 20 Jun 2025, 01:59:50

Sustained fever without evidence of infection can cause medical worries and lead to detailed investigation. Infection is still by far the most frequent explanation, but sustained unexplained fever can also be a sign of underlying autoimmune or rheumatological disease or, less frequently, some cancers. Kidney cancer, and more specifically renal cell carcinoma (RCC), is one of the malignancies that will sometimes present in this manner, although not most typically.
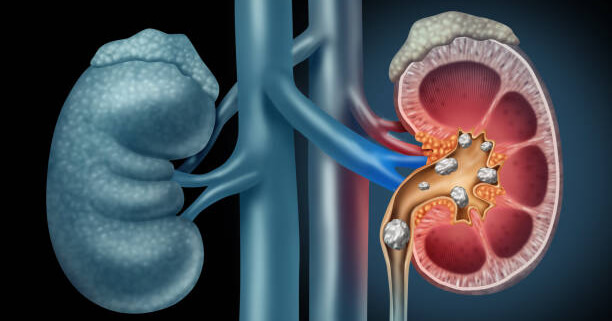
Dr Iti parikh, Consultant Medical Oncologist, Bhailal Amin General Hospital, Gujarat, explains that kidney cancer is most frequently asymptomatic in its early presentation. The majority of patients are diagnosed by chance when imaging is requested for unrelated reasons. The classic triad of RCC presentation – flank pain, haematuria (blood in urine), and abdominal mass – is present in only approximately 9–10% of patients. When they do occur, this triad most likely represents an advanced local stage of disease.
Fever per se occurs in about 20% of RCC. Fever is typically intermittent and often associated with systemic symptoms such as weight loss, night sweats, and generalised fatigue. The aetiology of fever in these instances is not infrequently unknown. When it appears, fever can indicate more extensive disease or systemic disease.
The most common type of kidney cancer is clear cell renal cell carcinoma, which occurs in 80–85% of cases. Diagnosis usually starts with an abdominal ultrasound that can detect suspicious lesions. But a CT scan is more specific and is able to differentiate between benign cysts and malignant tumours. PET-CT scans can be used in selected cases to further determine the extent of the disease.
If the cancer is limited, removal of the tumour by surgery is the treatment of choice. Depending on the size and site of the tumour, a partial nephrectomy
(excision of the tumour only) or a total nephrectomy (excision of the kidney) is done. Postoperatively, the excised tissue is subjected to histopathological analysis, and based on this, the stage of the cancer is established as well as whether further treatment is needed.
(excision of the tumour only) or a total nephrectomy (excision of the kidney) is done. Postoperatively, the excised tissue is subjected to histopathological analysis, and based on this, the stage of the cancer is established as well as whether further treatment is needed.
If the disease is advanced or metastatic at diagnosis, systemic therapy is the main treatment option. Immunotherapy delivered by IV infusion and oral tyrosine kinase inhibitors are the backbone of treatment. RCC is one of the few cancers that does not respond well to standard chemotherapy. RCC was one of the original cancers to see significant benefit from immunotherapy, and standard therapy protocols are firmly established.
There are several risk factors for kidney cancer. These include smoking, obesity, high blood pressure, and chronic kidney disease. Long-term use of some pain medications, such as NSAIDs, has also been found to be associated with increased risk. Exposure at work to chemicals such as cadmium, asbestos, and petroleum distillates has been associated in some studies. Family predisposition and food consumption of nitrites in processed foods might also increase risk.
RCC is more frequently diagnosed in males, with the average age of onset being 60–80 years. The average age at diagnosis is 64. About 65% of patients have the disease limited to the kidneys, 17–20% have regional lymph node involvement, and about 16% present with metastatic disease. Due to the recent developments in immunotherapy, the five-year survival for kidney cancer has significantly improved and is now nearing 75%.
Disclaimer: Tips and suggestions mentioned in the article are for general information purposes only and should not be construed as professional medical advice. Always consult your doctor or a dietician before starting any fitness programme or making any changes to your diet
No Comments For This Post, Be first to write a Comment.
Most viewed from Health










Todays Epaper

English Weekly


AIMIM News






Latest Urdu News
Most Viewed
May 26, 2020
Which cricket teams will reach the IPL 2026 finals?
Latest Videos View All
.jpg)
.jpg)
.jpg)



Like Us
Home
About Us
Advertise With Us
All Polls
Epaper Archives
Privacy Policy
Contact Us
Download Etemaad App
© 2026 Etemaad Daily News, All Rights Reserved.